Respiratory care devices used in oxygen therapy are essential in hospital settings, but may serve as reservoirs for pathogenic microorganisms if not properly maintained. Staphylococcus aureus is a major cause of healthcare-associated respiratory infections, on the other hand the emergence of antimicrobial resistance including multidrug resistance (MDR), presents significant treatment challenges. This study aimed at isolating S. aureus from respiratory care devices in regional referral hospitals and determining their antimicrobial susceptibility profile. A cross-sectional study was conducted from January to March 2024 in 29 regional referral hospitals across mainland Tanzania. A total of 231 samples were collected from humidifier water, device connectors, and reusable oxygen masks in Emergency departments, Intensive care units and Medical wards. Samples were enriched in Tryptic Soy Broth and cultured on Mannitol Salt Agar. Identification of S. aureus was performed using Gram staining, catalase tests and confirmation by PCR targeting the nuc gene. Antimicrobial susceptibility testing was conducted using the Kirby–Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) guidelines, 33rd edition. MDR was defined as resistance to at least three classes of antibiotic. Among the total isolates collected (N=231), 6.5% (n=15) were confirmed as S. aureus. There was no statistically significant difference in isolate distribution across hospital units or sample types (p > 0.05). High susceptibility was observed for ciprofloxacin and meropenem, while azithromycin showed the highest resistance among antibiotics tested while intermediate resistance was noted for erythromycin and trimethoprim. MDR was detected at 46.7% (n=7) of isolates, with variability observed across hospitals. Although the prevalence of S. aureus on respiratory care devices was low, the high proportion of MDR isolates highlights the need for continuous antimicrobial resistance surveillance, strict infection control practices, and strengthened antimicrobial stewardship programs in Tanzanian hospitals.
| Published in | Biomedical Sciences (Volume 12, Issue 1) |
| DOI | 10.11648/j.bs.20261201.13 |
| Page(s) | 17-25 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Staphylococcus aureus, Respiratory Care Devices, Antimicrobial Resistance, Multidrug Resistance, Oxygen Therapy
Hospital units | S. aureus | Chi-square | P-value | |
|---|---|---|---|---|
Present [n (%)] | Absent [n (%)] | |||
EMD | 7(8.9) | 72(91.1) | 1.524 | 0.480 |
ICU | 3(3.9) | 73(96.1) | ||
WARD | 5(6.6) | 71(93.4) | ||
Total | 15(6.5) | 216(93.5) | ||
Sample name | S. aureus | |||
|---|---|---|---|---|
Absent [n (%)] | Present [n (%)] | Chi-square | P-value | |
Connector (CS) | 80 (94.1) | 5 (5.9) | 1.6 | 0.497 |
Humidifier water (WS) | 81 (95.3) | 4 (4.7) | ||
Respirator (RS) | 55 (90.2) | 6 (9.8) | ||
MDR status | Frequency (n) | Percentage (%) |
|---|---|---|
Positive | 7 | 46.67 |
Negative | 8 | 53.33 |
Total | 15 | 100 |
ATCC | American Type Culture Collection |
CLSI | Clinical and Laboratory Standards Institute |
EMD | Emergence Department |
ICU | Intensive Care Unit |
MDR | Multi Drug Resistance |
PCR | Polymerase Chain Reaction |
RRH | Regional Referral Hospital |
NA | Nutrient Agar |
SPP | Species |
SPSS | Statistical Product and Service Solutions |
TAE | Tris-acetate-EDTA |
TMDA | Tanzania Medicines and Medical Devices Authority |
TSB | Tryptose Soy Broth |
USPNF | United States National Formulary |
| [1] | J. Belle et al., “Emerging Problems in Infectious Diseases Influenza preparedness in low-resource settings: a look at oxygen delivery in 12 African countries,” vol. 7, 2010. |
| [2] | D. Devices and G. Committee, “O XYGEN T HERAPY AND D ELIVERY D EVICES,” no. November, pp. 1–20, 2024. |
| [3] | B. R. O. Driscoll, L. S. Howard, J. Earis, V. Mak, and B. Thoracic, “BTS guideline for oxygen use in adults in healthcare and emergency settings,” 2017, |
| [4] | Z. W. Taye, Y. A. Abebil, T. Y. Akalu, G. M. Tessema, and E. B. Taye, “Incidence and determinants of nosocomial infection among hospital admitted adult chronic disease patients in University of Gondar Comprehensive Specialized Hospital, North–West Ethiopia, 2016–2020,” Front. Public Heal., vol. 11, 2023, |
| [5] | A. Combes, C. Luyt, J. Fagon, M. Wolff, J. Trouillet, and J. Chastre, “Early predictors for infection recurrence and death in patients with ventilator-associated pneumonia,” vol. 35, no. 1, 2007, |
| [6] | A. Hansmann, B. May, and H. Lang, “African Journal of Emergency Medicine Review of supplemental oxygen and respiratory support for paediatric emergency care in sub-Saharan Africa,” African J. Emerg. Med., vol. 7, no. November, pp. S10–S19, 2017, |
| [7] | S. Jadhav, T. Sahasrabudhe, V. Kalley, and N. Gandham, “The Microbial Colonization Profile of Respiratory Devices and the Significance of the Role of Disinfection: A Blinded Study,” 2013, |
| [8] | R. Touaitia, A. Mairi, N. A. Ibrahim, N. S. Basher, T. Idres, and A. Touati, “Staphylococcus aureus: A Review of the Pathogenesis and Virulence Mechanisms,” vol. 2, pp. 1–37, 2025. |
| [9] | T. Sandle, Pharmaceutical Microbiology. 2016. |
| [10] | C. J. Murray et al., “Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis,” Lancet, vol. 399, no. 10325, pp. 629–655, 2022, |
| [11] | A. H. Hasanpour, M. Sepidarkish, A. Mollalo, A. Ardekani, and M. Almukhtar, “The global prevalence of methicillin - resistant Staphylococcus aureus colonization in residents of elderly care centers: a systematic review and meta - analysis,” Antimicrob. Resist. Infect. Control, vol. 6, pp. 1–11, 2023, |
| [12] | S. Stefani and A. Goglio, “International Journal of Infectious Diseases Methicillin-resistant Staphylococcus aureus: related infections and antibiotic resistance,” vol. 4, pp. 19–22, 2010, |
| [13] | X. Ba et al., “Novel mutations in penicillin-binding protein genes in clinical Staphylococcus aureus isolates that are methicillin resistant on susceptibility testing, but lack the mec gene,” no. November 2013, pp. 594–597, 2014, |
| [14] | T. Lancet and I. Diseases, “Leading Edge A new dawn for global health ?,” Lancet Infect. Dis., vol. 9, no. 2, p. 73, 2009, |
| [15] | T. C. Threat and M. Staphylococcus, “The Continuing Threat of Methicillin-Resistant Staphylococcus aureus,” 2019. |
| [16] | P. S. Ho, “Antibacterial Discovery: 21st Century Challenges,” 2020. |
| [17] | R. Gosling et al., “Annals of Tropical Medicine & Parasitology Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania Prevalence of hospital-acquired infections in a tertiary referral hospital in northern Tanzania,” vol. 4983, no. April, 2017, |
| [18] | O. Tajik, J. Golzar, and S. Noor, “Purposive Sampling,” vol. 2, no. November, pp. 1–9, 2024. |
| [19] | United States Pharmacopeia and the National Formulary <71> STERILITY TESTS, 2024. |
| [20] | B. Y. Khudaier, I. T. Anad, and B. A. Abbas, “ISOLATION OF Staphylococcus aureus FROM BUFFALO MILK IN BASRA GOVERNORATE AND DETECTION OF THEIR ANTIBIOTIC SUSCEPTIBILITY,” vol. 1, no. 1, pp. 1–11, 2014. |
| [21] | A. C. Smith and M. A. Hussey, “Gram Stain Protocols,” no. September 2005, pp. 1–9, 2016. |
| [22] | K. Reiner, “Catalase Test Protocol,” no. November 2010, pp. 1–9, 2016. |
| [23] | S. Hassanzadeh, M. R. Pourmand, and D. Afshar, “Letter to the Editor TENT: A Rapid DNA Extraction Method of Staphylococcus aureus,” vol. 45, no. 8, pp. 1093–1095, 2016. |
| [24] | S. Ghazi and A. Hariri, “2.1. Isolation and Identification of S. aureus,” 2021. |
| [25] | Clinical and Laboratory Standards Institute: Performance Standards for Antimicrobial Susceptibility Testing CLSI, “M100 Ed 35 pp. 1–38, 2025. |
| [26] | M. O. F. Health and C. Development, “STANDARD TREATMENT GUIDELINES AND NATIONAL ESSENTIAL MEDICINES LIST FOR STANDARD TREATMENT GUIDELINES AND NATIONAL ESSENTIAL MEDICINES LIST FOR,” 2021. |
| [27] | J. S. L. Iib. and A. L. B. et al Limbago, CLSI, performance standards for antimicrobial susceptibility testing 33rd Edition. 2024. |
| [28] | S. Y. C. Tong, J. S. Davis, E. Eichenberger, T. L. Holland, and V. G. Fowler, “Staphylococcus aureus Infections: Epidemiology, Pathophysiology, Clinical Manifestations, and Management,” vol. 28, no. 3, pp. 603–661, 2015, |
| [29] | A. A. Mahfouz, H. S. Said, and S. M. Elfeky, “Inhibition of Erythromycin and Erythromycin-Induced Resistance among Staphylococcus aureus Clinical Isolates,” 2023. |
| [30] | H. M. Naimi, H. Rasekh, A. Z. Noori, and M. A. Bahaduri, “Determination of antimicrobial susceptibility patterns in Staphylococcus aureus strains recovered from patients at two main health facilities in Kabul,” pp. 1–7, 2017, |
| [31] | I. A. Ghannam et al., “A nationwide cross-sectional study of antimicrobial resistance in Palestinian hospitals: insights from 10, 000 clinical isolates,” vol. 0, 2025. |
APA Style
Mtenga, A. B., Fimbo, A. M., Mwambene, S. J., Kasekwa, E. E., Kombo, S. B., et al. (2026). Isolation and Antimicrobial Resistance of Staphylococcus aureus Associated with Respiratory Devices. Biomedical Sciences, 12(1), 17-25. https://doi.org/10.11648/j.bs.20261201.13
ACS Style
Mtenga, A. B.; Fimbo, A. M.; Mwambene, S. J.; Kasekwa, E. E.; Kombo, S. B., et al. Isolation and Antimicrobial Resistance of Staphylococcus aureus Associated with Respiratory Devices. Biomed. Sci. 2026, 12(1), 17-25. doi: 10.11648/j.bs.20261201.13
@article{10.11648/j.bs.20261201.13,
author = {Adelard Bartholomew Mtenga and Adam Mitangu Fimbo and Saxon Joseph Mwambene and Elizabeth Erasto Kasekwa and Shaban Bikiz Kombo and Kissa Watson Mwamwitwa and Raphael Zozimus Sangeda and Danstan Hipolite Shewiyo},
title = {Isolation and Antimicrobial Resistance of Staphylococcus aureus Associated with Respiratory Devices},
journal = {Biomedical Sciences},
volume = {12},
number = {1},
pages = {17-25},
doi = {10.11648/j.bs.20261201.13},
url = {https://doi.org/10.11648/j.bs.20261201.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.bs.20261201.13},
abstract = {Respiratory care devices used in oxygen therapy are essential in hospital settings, but may serve as reservoirs for pathogenic microorganisms if not properly maintained. Staphylococcus aureus is a major cause of healthcare-associated respiratory infections, on the other hand the emergence of antimicrobial resistance including multidrug resistance (MDR), presents significant treatment challenges. This study aimed at isolating S. aureus from respiratory care devices in regional referral hospitals and determining their antimicrobial susceptibility profile. A cross-sectional study was conducted from January to March 2024 in 29 regional referral hospitals across mainland Tanzania. A total of 231 samples were collected from humidifier water, device connectors, and reusable oxygen masks in Emergency departments, Intensive care units and Medical wards. Samples were enriched in Tryptic Soy Broth and cultured on Mannitol Salt Agar. Identification of S. aureus was performed using Gram staining, catalase tests and confirmation by PCR targeting the nuc gene. Antimicrobial susceptibility testing was conducted using the Kirby–Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) guidelines, 33rd edition. MDR was defined as resistance to at least three classes of antibiotic. Among the total isolates collected (N=231), 6.5% (n=15) were confirmed as S. aureus. There was no statistically significant difference in isolate distribution across hospital units or sample types (p > 0.05). High susceptibility was observed for ciprofloxacin and meropenem, while azithromycin showed the highest resistance among antibiotics tested while intermediate resistance was noted for erythromycin and trimethoprim. MDR was detected at 46.7% (n=7) of isolates, with variability observed across hospitals. Although the prevalence of S. aureus on respiratory care devices was low, the high proportion of MDR isolates highlights the need for continuous antimicrobial resistance surveillance, strict infection control practices, and strengthened antimicrobial stewardship programs in Tanzanian hospitals.},
year = {2026}
}
TY - JOUR T1 - Isolation and Antimicrobial Resistance of Staphylococcus aureus Associated with Respiratory Devices AU - Adelard Bartholomew Mtenga AU - Adam Mitangu Fimbo AU - Saxon Joseph Mwambene AU - Elizabeth Erasto Kasekwa AU - Shaban Bikiz Kombo AU - Kissa Watson Mwamwitwa AU - Raphael Zozimus Sangeda AU - Danstan Hipolite Shewiyo Y1 - 2026/03/28 PY - 2026 N1 - https://doi.org/10.11648/j.bs.20261201.13 DO - 10.11648/j.bs.20261201.13 T2 - Biomedical Sciences JF - Biomedical Sciences JO - Biomedical Sciences SP - 17 EP - 25 PB - Science Publishing Group SN - 2575-3932 UR - https://doi.org/10.11648/j.bs.20261201.13 AB - Respiratory care devices used in oxygen therapy are essential in hospital settings, but may serve as reservoirs for pathogenic microorganisms if not properly maintained. Staphylococcus aureus is a major cause of healthcare-associated respiratory infections, on the other hand the emergence of antimicrobial resistance including multidrug resistance (MDR), presents significant treatment challenges. This study aimed at isolating S. aureus from respiratory care devices in regional referral hospitals and determining their antimicrobial susceptibility profile. A cross-sectional study was conducted from January to March 2024 in 29 regional referral hospitals across mainland Tanzania. A total of 231 samples were collected from humidifier water, device connectors, and reusable oxygen masks in Emergency departments, Intensive care units and Medical wards. Samples were enriched in Tryptic Soy Broth and cultured on Mannitol Salt Agar. Identification of S. aureus was performed using Gram staining, catalase tests and confirmation by PCR targeting the nuc gene. Antimicrobial susceptibility testing was conducted using the Kirby–Bauer disk diffusion method according to Clinical and Laboratory Standards Institute (CLSI) guidelines, 33rd edition. MDR was defined as resistance to at least three classes of antibiotic. Among the total isolates collected (N=231), 6.5% (n=15) were confirmed as S. aureus. There was no statistically significant difference in isolate distribution across hospital units or sample types (p > 0.05). High susceptibility was observed for ciprofloxacin and meropenem, while azithromycin showed the highest resistance among antibiotics tested while intermediate resistance was noted for erythromycin and trimethoprim. MDR was detected at 46.7% (n=7) of isolates, with variability observed across hospitals. Although the prevalence of S. aureus on respiratory care devices was low, the high proportion of MDR isolates highlights the need for continuous antimicrobial resistance surveillance, strict infection control practices, and strengthened antimicrobial stewardship programs in Tanzanian hospitals. VL - 12 IS - 1 ER -
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania;Department of Pharmaceutical Microbiology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Department of Pharmaceutical Microbiology, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
Laboratory Services, Tanzania Medicines and Medical Devices Authority, Dar es Salaam, Tanzania
Figure 1. A map showing the Tanzania regions included in the study.
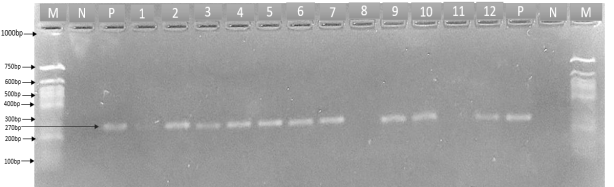
Figure 2. Agarose gel electrophoresis of PCR products. Lane M: 50 bp DNA ladder (50–1000 bp); Lane N: Negative control; Lane P: positive control; Lanes 1–12: test samples. A distinct band at approximately 270 bp was observed in the positive control and positive test samples.
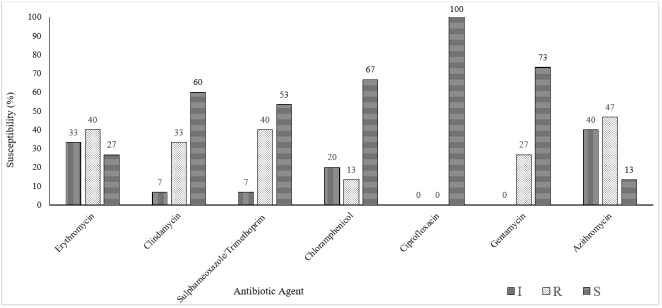
Figure 3. Antibiotic susceptibility patterns of S. aureus against selected antibiotics.
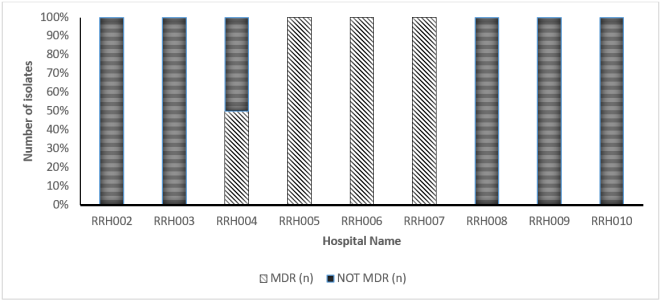
Figure 4. Multidrug Resistance profiles of S. aureus across hospitals.

